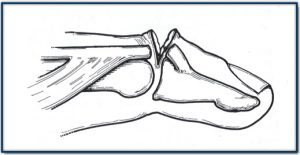
Mallet finger presents as a flexion deformity of the distal interphalangeal (DIP) joint with loss of active extension.
Mallet finger deformities can result from closed or open injuries.
Closed – The usual mechanism of a closed is a sudden forced flexion of the DIP joint. This typically occurs in various ball sports when the tip of the finger is struck by a ball. Most commonly this causes a traumatic rupture of the extensor tendon as it inserts into the dorsal lip of the base of the distal phalanx. It can also cause distal phalangeal avulsion fractures of various sizes.
Open – Any laceration or open wound overlying the extensor aspect of the DIP joint can result in a mallet finger.
People with closed mallet finger may delay seeking medical attention – even though they may be in a great deal of pain – simply because they can still use their hand.
Symptoms include:
Pain, swelling and bruising overlying the extensor aspect of the DIP joint immediately after the injury.
This is associated with an inability to completely extend the DIP joint.
An xray with lateral views should be performed to establish whether an avulsion fracture is present.
Untreated mallet injuries will result in a permanent flexion deformity of the DIP joint with secondary joint degeneration.

Typical bruising overlying the extensor aspect of the DIP joint

Typical avulsion fracture seen in a closed mallet injury
Closed Mallet Finger Injuries
These injuries have tendon ruptures or small bony avulsion fractures require splinting, and this can be either “external” (non-surgical) or “internal” (surgical K-wiring).
External Splinting – A number of different splints can be used as long as they maintain the DIP joint in hyperextension and allow normal flexion of the PIP joint.
This involves externally splinting the DIP joint in slight hyperextension for a period of 8 weeks to allow the tendon or fracture to heal. This is followed by a period of night splinting for 2 weeks. However, for such an approach to work the patient must be totally compliant. The patient must wear the splint 24 hours a day and resist the temptation to take it off to see how the injury is healing.
The splint should be comfortable, and as the swelling settles the splint will need to be altered so that it is a “snug” fit. It should be removed regularly for hygiene, massage and skin care. It is essential that the DIP joint remains in extension whilst this is performed.
Internal Splinting – This involves a minor surgical procedure to place a K-wire along the length of the distal and middle phalanx immobilizing the DIP joint is slight hyperextension. The wire is cut so that it is kept in a subdermal position to minimise the risk of any infection. Another minor procedure is required at about 8 weeks post-insertion to remove the K-wire. This option eliminates the concern of inadvertent premature flexion of the DIP joint which would jeopardise the treatment.

Surgical placement of a K-wire to immobilize the DIP joint in extension
Open injuries or those with large avulsion fractures require surgical intervention.
Open injuries require thorough debridement including washout of a likely open joint and an appropriate tendon repair.
Large avulsion fractures usually require treatment with K-wire fixation or very occasionally internal screw fixation.
After the splintage (internal or external), the finger is gently exercised under hand therapist guidance. It can take several months before maximal flexion to be achieved and this may not be completely normal. One should avoid forcibly attempting to flex the digit immediately after the splint has been removed as this risks rupturing the tendon again.
Additionally, a slight extensor lag may exist post-treatment.
If a lag is still present after the 8 weeks, then the splint should be re-applied continuosly for a further 3 weeks and the patient reviewed again.
© Copyright 2019 Sydney Hand Surgery Pty Ltd