Injured components may include skin, bone, nail, nailbed, tendon, and the pulp – the padded area of the fingertip. The skin on the palm side of our fingertips is highly specialised with a high density of nerve endings. These nerve endings enable the fine sensation we have in our fingertips.
Fingertip injuries are one of the most frequent problems encountered by the reconstructive hand surgeon. The fingertips are exposed in many of our activities. They can be crushed, such as by a closing door, a hammer, or a heavy object dropped onto the finger. They can be cut with a knife or power tool, such as a saw, sander or lawnmower.
It is important to know how the injury occurred, and about any medical problems, as these can factor into deciding about treatment. Examination reveals the extent of tissue injury. Specifically, amount of skin and pulp (padding) loss and any bone exposure is important in determining the reconstructive option. Sensation and circulation of the tip are assessed. Mobility of the tip is also assessed to determine flexor and extensor tendon function. X-rays are usually required to determine distal phalangeal status.
The aim of fingertip reconstruction is to create a well padded, sensate fingertip to allow normal hand functioning. Regardless of the injury type or reconstruction option employed, healing usually takes a minimum of 6 weeks to allow healing and wound maturation. Hand therapy is a vital part of the post-operative management.
If just skin is removed and the defect is less than a centimeter in diameter, it is often possible to treat these injuries with simple dressing changes.
When there is a small amount of bone exposed at the tip, it can occasionally be trimmed back slightly and treated with dressings. For larger skin defects, skin grafting is occasionally recommended. Smaller grafts can be obtained from the little finger side of the hand (hypothenar eminence). Larger grafts may be harvested from the forearm or groin. If the nailbed is injured, it is repaired.
When patients lose skin and padding with bone exposure, the injury usually needs to be covered with a flap of skin that has some soft tissue with it for padding. Small wounds on the tip of the finger may be covered with a flap from the injured finger (eg. Atasoy flap).
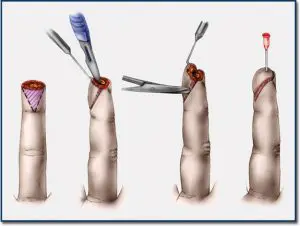
a. Local volar flap for fingertip reconstruction – Atasoy flap

b. Fingertip injury with loss of skin and pulp with associated bone exposure.

c. Reconstruction using a local flap of skin and padding.

Results after 6 weeks
Larger wounds, such as those that result in substantial loss of the pulp, require a flap that is elevated from an adjacent finger or other source (eg. cross-finger flap). The flap remains attached so that it has blood supply from its donor site while it develops a new blood supply from the injured digit. After a few weeks the flap has developed its own blood supply from its location in the injured finger and can then be safely divided from its origin and fully inset into the wound. A skin graft is used to cover the donor site defect.
Fractures of the distal phalanx (bone in the tip of the finger) are common. Very small fractures of the end or tuft of the bone usually do not require formal treatment. Repair of the soft tissue, such as the nail bed, usually re-aligns and stabilises these bone fragments. Fractures closer to the joint may require a splint or even a temporary wire/pin to hold the bone fragments in proper position. If the damage is too severe, amputation of the fingertip may be necessary.
As stated earlier, aggressive post-operative hand therapy is vital for wound management and to ensure maximal return of function. Fingertip sensitivity is common and may last for many months. Depending on the reconstruction necessary, sometimes the feeling in the fingertip is limited. The contour may be slightly distorted. Stiffness can be a concern, especially if a flap is needed. There also may be some deformity at the donor site of a graft or flap. The quality of any associated nail bed reconstruction also impacts on the final result of fingertip reconstructions.
© Copyright 2019 Sydney Hand Surgery Pty Ltd