de Quervain’s tenosynovitis is a condition that causes pain on the inside of the wrist and forearm just above the thumb. It is a common problem affecting the wrist and is usually easy to diagnose.
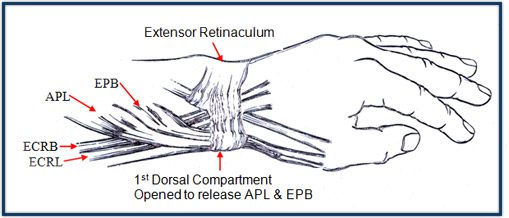
de Quervain’s tenosynovitis affects two thumb tendons. These tendons are called the abductor pollicis longus (APL) and the extensor pollicis brevis (EPB).
On their way to the thumb, the APL and EPB tendons travel side by side along thumb side of the wrist. They pass through a tunnel near the end of the radius bone of the forearm. The tunnel holds the tendons in place, like the guide on a fishing pole.
This tunnel is lined with a slippery coating called tenosynovium. The tenosynovium is a slippery covering that allows the two tendons to glide easily back and forth as they move the thumb. Inflammation of the tenosynovium and tendon is called tenosynovitis.
The inflammation causes the compartment (a tunnel or a sheath) around the tendons to swell and enlarge, making thumb and wrist movement painful. Making a fist, grasping or holding objects are common painful movements with de Quervain’s tendonitis.
Multiple small branches of the radial nerve pass through the region at the base of the thumb and are occasionally involved in the inflammation in this region.
Usually highly repetitive movements of the wrist and thumb such as lifting, grasping and twisting may lead to the inflammation of tenosynovitis. It is very common in mothers with young babies. It may also occur in more generalised conditions such as rheumatoid arthritis and diabetes.
A wrist fracture can also predispose a patient to de Quervain’s tendonitis, because of increased stresses across the tendons.
De Quervain’s tenosynovitis causes pain and tenderness at the thumb side of the wrist. The pain may appear either gradually or suddenly, and pain is located at the first dorsal compartment at the wrist. Pain may radiate down the thumb or up the forearm. Hand and thumb motion increases pain, especially with forceful grasping or twisting. Swelling and even redness over the base of the thumb may occur. Due to the pain and swelling, motion such as pinching may be difficult. Irritation of the nerve lying on top of the tendon sheath may cause numbness on the back of the thumb and index finger. As the friction increases, the two tendons may actually begin to squeak as they move through the constricted tunnel. This noise is called crepitus. When severe there may be catching or snapping with thumb movement.
De Quervain’s tenosynovitis is diagnosed based on the typical appearance, location of pain, and tenderness of the affected wrist – directly over the first dorsal compartment of the wrist. The Finkelstein test is one of the best ways to make the diagnosis. The patient makes a fist with the fingers clasped over the thumb. The wrist is then bent in the direction of the little finger. This maneuver is very painful for the person with de Quervain’s tenosynovitis.
The diagnosis is usually made on clinical grounds. However an ultrasound is often performed and demonstrates tenosynovitis of the APL and EPB tendons.
NON OPERATIVE
Each non-operative treatment helps reduce the swelling, which typically relieves pain over time. In some cases, simply stopping the aggravating activities may allow the symptoms to go away on their own.
Rest or altering activities – changing or stopping all activities that cause symptoms should be tried. Taking frequent breaks when performing repeated hand and thumb actions is important. Avoiding repetitive hand motions, such as heavy grasping, wringing, or turning and twisting movements of the wrist. May benefit from early occupational therapist intervention
Anti-Inflammatory tablets – may also help control the swelling of the tenosynovium and ease symptoms.
Anti-Inflammatory creams
Splints – thumb-spica – This splint keeps the wrist and lower joints of the thumb from moving. The splint allows the APL and EPB tendons to rest, giving them a chance to begin to heal.
Cortisone Injection – Cortisone injection is extremely effective and is generally the optimal treatment (in combination with splinting).
Reserved for those patients who have failed non-operative measures including at least one cortisone injection.
The goal of surgery is to give the tendons more space so they no longer rub on the inside of the tunnel and thus allow the inflammation to settle. To do this, surgical release of the roof of the tunnel is performed. This opens up the tunnel, creating more space for the inflamed APL and EPB tendons. This breaks the vicious cycle where the tight space causes more inflammation. The tunnel will eventually heal closed, but it will be larger than before.
This surgery can usually be done as a day only procedure. It can be done using a general anesthetic, or a local anaesthetic with sedation.
To perform the release, a small incision along the thumb side of the wrist allows access to the tunnel. Care must be taken to avoid injury to the overlying superficial radial nerve.
A splint is usually applied for the immediate post-operative period.
If conservative treatments are successful, improvements should be seen in four to six weeks. Continued use of the thumb splint may be necessary to control symptoms. Permanently modified tasks that reduce the repeated motions of the wrist and thumb may be required.
Rehabilitation is more involved after surgery. Full recovery could take several months.
Pain and symptoms generally begin to improve after surgery, but tenderness in the area of the incision may persist for several months. Occupational therapy for six to eight weeks is usually required. Therapists attend to wound and scar management issues and also use a series of exercise to encourage the thumb tendons to glide easily within tunnel. As therapy progresses, other exercises are used to strengthen and stabilise the muscles and joints in the hand and thumb. Most importantly, the therapist provides careful instructions and guidelines to minimise the chance if recurrence.
The patient can generally return to full function after the inflammation quiets down with treatment.
© Copyright 2019 Sydney Hand Surgery Pty Ltd